Hiking Health: staying fit and safe on the trails
Keeping yourself fit and healthy on your hikes can be hard.
Countless dangers await and, if you’re not prepared, you could end up a casualty or worse!
Don’t worry, this page is for you. Below, you’ll find the most informative resource for every possible environment: from long hikes at sea level to high altitude pursuits. Your health and safety are important to us – we want to meet you on the trail someday!
You’ll find information from a medical and non-medical perspective.
The sections on altitude and the cold contain practical information and advice which could easily save your life on a mountain, and so have been arranged into pragmatic, easily digestible pieces.
We hope that the information we have provided is useful on the trails, in the mountains and forests, or wherever else your journeys take you.
Have a safe, enjoyable trip.
Check out this page for other common injuries hikers experience.
Let’s get this hiking health guide moving…
Hiking at altitude
Altitude is defined as the height above sea level. In essence, there are three altitude categories, namely high altitude (1500 – 3500m), very high altitude (3500- 5500m), and extreme altitude (5500m and above). Illnesses and ailments in high altitudes result from a lack of enough oxygen. Overall, oxygen constitutes 20% of the overall atmospheric gases. In high altitudes, however, the molecules spread more and become less accessible due to decreased pressure. As such, your body must work harder to obtain the little amount available. At the extreme altitude, the available oxygen percentage is less than that of the sea level. In such areas, the body acclimatizes and becomes accustomed to the new conditions and climate, allowing you to survive there for a couple of days.
Here are the common physiological changes resulting from altitude
- Breathing fast (Hyperventilation)
- Shortage of breath, especially when exerting
- Alteration of breathing patterns in sleep
- Frequent urination
- Disturbed sleep
- Abnormal dreams
Your oxygen-depleted body can utilize up to 5000 calories per day at high altitudes. Still, you can’t eat too much since sickness is prevalent, and the food may be typically unappetizing. In order to adjust for the lower oxygen levels available in the air, your body trains to increase the depth and rate of breathing. The kidneys change their way of working to enable the blood to become alkaline.
As a result, the blood absorbs and carries more oxygen throughout the body. To get oxygen to all of the body’s critical organs, the resting heartbeat rate is elevated. Since the blood, notably the red blood cells, must work extra, the body eventually generates more, resulting in a more efficient circulatory system.
Acute Mountain Sickness
Acute Mountain Sickness (AMS) refers to the reaction of the body to a lack of oxygen, induced by climbing faster than acclimatization. It is still unknown what conditions trigger specific types of AMS. Therefore we can’t forecast who will or will not get it.
Despite its widespread and public awareness, the condition continues to perplex scientists after all these years. From our understanding, AMS is thought to be a result of brain tissue enlargement due to a shortage of oxygen or hypoxic stress.
Since we understand so little about this ailment, it’s typical to treat any symptom as sickness at altitude. Most people believe that having a headache at altitude is normal, whereas, in fact, it is extremely rare. That said, if you have plans of spending time at altitude, it’s a great idea to be aware of the AMS symptoms. It’s been compared to a hangover by some people.
Besides headache, other symptoms of AMS include the following:
- Weakness or fatigue
- Nausea or vomiting
- Loss of appetite
- Mood swings
- Interrupted sleep patterns
- Disorientation and confusion
- unable to perform motor actions
- Dizziness, faint and light-headed feeling
- Apathy
- A deep inner chill
- Impaired memory
All the above symptoms can be categorized on a scale of mild to severe, and Lake Louise offers a questionnaire to help determine the phases of AMS. At high or extreme altitudes, a headache generally starts on the second or third day. A throb in the forehead and/or back of the head characterizes the headache, which ranges from mild to severe. It’s usually worse in the morning and at night. Bending over or straining makes it worse.
In case you merely have a headache, it’s advisable to test for AMS using the elimination method. Drink at least one liter of water because dehydration is the leading cause of headaches and if possible, take a low-dose pain reliever like paracetamol. If the pain completely goes away and no other symptoms occur, it’s safe to presume that your headache was not caused by AMS and that climbing can continue.
Severe Acute Mountain Sickness
AMS in its most severe form can affect your lungs, nervous system, heart, and muscles, causing more severe symptoms. For instance, if your brain swells, you may have disorientation. As a result of the fluid in your lungs, you may experience shortness of breath.
Symptoms of severe AMS include:
- Chest congestion
- Skin discoloration and pale complexion
- Social withdrawal
Periodic Breathing
A condition known as “periodic breathing,” which occurs when a person’s typical sleeping pattern is disrupted, is also associated with AMS. The person will have fits of insomnia interspersed with fitful dreams. Their respiratory pattern is disrupted as well, with intervals of deep and rapid breathing followed by times of no breathing. This can last up to 15 seconds. It might improve significantly with acclimatization, though it rarely goes away until the descent.
Periodic breathing can create anxiety in two ways: first, for someone who wakes up and realizes they cannot breathe, or for an individual who wakes up in a stage of hyperventilation and believes they have High Altitude Pulmonary Edema (HAPE). However, an individual who wakes up and discovers their companion has ceased breathing may have a frightening experience. In such a situation, the most advisable thing to do is to be patient until the respiration is self-regulated again since the periodic breathing cycles will certainly continue until the person wakes up.
The best method to deal with AMS is to prevent it in the first place. Ascending should be gradual to allow the body to acclimate. Although each person is unique, the following measures should protect the most individuals against AMS:
- When you are past 3000m, the altitude should not dramatically change in a day. This implies that you should not ascend more than 300 meters each day.
- For each 1000m above 3000m, spend two nights around the exact altitude.
Here are some of the things you must avoid, as they slow down the rate of breathing:
- Sleeping pills
- Alcohol
- Tobacco
- Narcotic painkillers
If AMS occurs, however, there are a few simple measures to help avert fatality. Before the ascent, it is critical for all parties to be aware of the risks since ignorance is majorly the cause of disease.
- Do not leave an AMS patient alone.
- Avoid climbing any further. This has the potential to be fatal, as the symptoms are just going to become worse.
- If feasible, descend to the point where you last felt safe. AMS symptoms are likely to fade away much faster.
- In case symptoms persist, remain at the exact altitude until the body acclimatizes. Only then can the climbing begin again.
- Rest is vital
- Consume plenty of water to stay hydrated.
If you have any serious AMS symptoms, kindly seek emergency medical help right away. Address the problem before it worsens, as it will be much easier to treat. Moreover, in case your doctor concludes that you have fluids in your lungs or brain swelling, you will need to be admitted to the hospital.
Health precautions
A comprehensive examination with a professional GP is essential prior to departure in order to identify and advise on any potential concerns you may have during your travel. This is especially critical for those who have previously experienced blood pressure, heart or lung problems, as well as those who have ongoing medical conditions.
Children
When going with children to high altitudes, you must exercise extreme caution and keep a close eye on them for any aberrant behavior, as small children often have difficulties expressing their emotions. Younger individuals often adapt to the high altitude more slowly, according to research, but no extensive studies on the safest altitude for children have been conducted. As such, doctors propose a maximum height of 3000m for children. However, a lot of children have safely ascended Kala Pattar, which stands at 5560 meters.
Teenagers
Currently, no evidence proves that teenagers adjust to high altitudes slower than adults, yet they may be at a higher risk than adults due to behavioral tendencies. For instance, teenagers might be highly competitive, refusing to give up throughout the trip. This is more likely to happen on school tours, where peers are involved.
Older travellers
Many elderly people, including those over the retirement age, have climbed some of the most iconic mountains in the world. In essence, older people do not have to be prevented from climbing because of their age; rather, it is an individual’s fitness level that prevents them from participating. Age should just highlight the importance of maintaining a healthy fitness level.
Heart Conditions
There are no studies regarding heart attacks on hikes, or at high altitudes. It seems logical given the altitude’s effects on the body and the fact that the amount of effort required is more compared to that of sea level. If you’re concerned, see a doctor.
High Blood Pressure
High blood pressure ( Hypertension) is highly likely to be a problem at altitude, thus seeing a certified doctor is crucial, particularly one who is familiar with your medical history. They will determine whether it is safe to ascend.
Epilepsy
At high or extreme altitudes, there is a modest rise in the risk of seizures, but based on the condition’s severity, you may be able to continue. In case of an emergency, your group should be prepared and alert.
Diabetes
Higher exertion while ascending changes the levels of insulin and carbohydrate in the blood; therefore, it’s critical to keep an eye on glucose levels and keep blood sugar levels under control. Make sure everyone in your immediate vicinity is aware of the situation and what to do if an emergency occurs.
Chest Infections in the Past
Individuals who are more vulnerable to chest infections are at a higher risk of becoming unwell since even healthy people might acquire chest problems when they travel to higher altitudes. Any prescription medicine should be brought with you, and based on the severity; you should start taking it as soon as possible. Kindly consult your physician.
Asthma
Most asthmatics discover that their asthma improves when they are at a higher altitude than when they are at sea level. This is due to the fact that there are fewer chemicals in the air that irritate asthma. Nonetheless, it’s a great idea to keep all medication close to reach, such as around your neck or in a zipped pocket. Make those in your group aware of the situation and what they should do if an attack occurs.
Pregnancy
Because the consequences of low oxygen and altitude on an unborn fetus are yet to be investigated, it’s probably better to avoid ascending if you’re expectant. Furthermore, professional care is frequently required, which may be challenging to obtain at such a high elevation.
High Altitude Cerebral Edema
HACE (High Altitude Cerebral Edema) is a potentially catastrophic variant of AMS in which the brain swells and ceases to function normally. This can take hold for hours once it’s been started, and most individuals aren’t even aware they’re sick. Due to the extreme rapidity with which this occurs, climbers must be aware of the warning indications. They are as follows:
- Fatigue
- Confusion
- Behavioural changes
- Ataxia, a term for a “drunk stagger.” Have the individual walk in a straight line on a flat surface without wearing heavy boots or carrying a backpack as a test for this condition. Treat them like HACE patients if they miss the line, stumble, or fall down.
- Strenuous speaking
- Hallucinations
- Vomiting
- Blindness
- Limb paralysis
- Unconsciousness
- Seizure
- Complete paralysis
- Coma
Treatment
The treatment is straightforward: quick descending. Even though HACE begins at night, descending must begin quickly because any delay could be catastrophic. This may be challenging since the patient will be disoriented and stagger, necessitating the assistance of others. Descending should be to the point where the individual last felt well after waking up. Because cases of HACE usually only emerge whenever someone with mild AMS progresses upwards, this is most likely where the individual slept the previous two nights. It must be at least 500 meters long. Maximum rest is recommended once a lower position has been reached.
If the individual has descended far enough in a short amount of time, recovery is typically possible. The drunken stagger may, however, last a few days. If the symptoms go away, the climbing can continue at a more moderate speed.
Basic First Aid skills
Now we’ve detailed some of the common injuries and conditions experienced, it’s time to look at some of the basic first aid skills Jake and I have learned over the years.
How to give First Aid
When you’re hiking through regions where professional care is difficult to reach it is important to be trained in the basics of first aid. Along with a good first aid kit, this section should help to prepare you for most emergencies. Jake and I have both been trained to basic medical standards and we highly recommend you get the same training before heading off on a journey. Even a simple First Aid course might mean the difference between life and death.
This post is part of our ongoing list of hiking skills and gear you’ll need when you hit the trails.
Enjoy and share your thoughts with us.
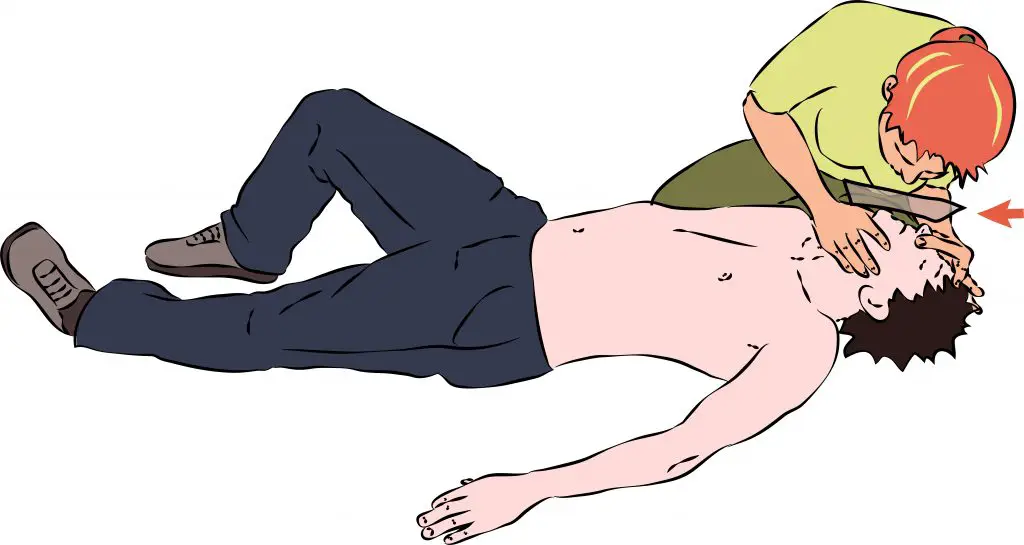
Mouth to Mouth Resuscitation
Humans can stop breathing for many reasons including, a heart attack, drowning, electric shocks and suffocation. Diagnosing a heart attack can be hard if you’re medically trained, but some signs to look out for include a blue-grey tint to the skin, particularly the face, and no ‘rise and fall’ chest movement. If the affected person has stopped breathing, mouth-to-mouth resuscitation will need to be performed. The method you use will be different for different situations, as shown below:
Adults
Mouth to Mouth
What do you do when the heart stops? Don’t panic, it can forced back into motion again using CPR. This involves a series of chest compressions combined with the ventilation techniques described above.
- Open the patient’s mouth and if necessary remove blockages from the airway carefully using your finger as a hook.
- Next, place two fingers under the patient’s chin and a hand on the forehead, then carefully move to tilt the person’s head back.
- Using your thumb and forefinger, pinch their nostrils closed, breathe in and place your mouth on theirs.
- Breathe hard, forcing their chest to rise.
- Remove your mouth to allow the chest to fall.
- Turn your head away as the patient exhales, and take a deep breath.
- Give 10 breaths in quick succession and then check for a pulse. If you can’t find one, then give CPR.
- Continue the method at 10 breaths per minute.
Mouth to Nose
If the patient has facial injuries that prevent mouth-to-mouth resuscitation, we suggest using this next method
- Use steps 1-2 from above.
- Use your hand to hold the person’s mouth closed, take a deep breath and place your mouth around the person’s nose.
- Breathe into their nostrils quite forcefully until the chest rises.
- Remove your hand and mouth to allow the air to escape.
- As before, turn your head away and take a deep breath in readiness for the next step.
- Continue at 10 breaths per minute.
Sometimes you’ll come across facial injuries that make mouth-to-mouth resuscitation ineffective until treated. For example, puncture wounds to the cheeks will allow air to escape and need to be sealed. Plastic wrappers can be used as a way of sealing facial and chest wounds.
Children
Mouth to Mouth and Nose for a Baby (under 1 year)
- Open the child’s mouth and using your pinky finger gently remove any blockages with a finger.
- Place your mouth around the baby’s nose and mouth.
- Gently blow air into the baby’s lungs whilst watching its chest. Be gentle! Children’s lungs are far smaller than an adult’s and breathing in a full breath could cause damage.
- As soon as the chest rises, stop and let the air escape.
- Repeat to give one breath every 3 seconds.
- After 20 breaths check the pulse.
- If the heartbeat is lower than 60 bpm then start CPR, and if it is above this then continue ventilation until help arrives.
Mouth to Mouth for a Child (over 1 year of age)
- Use steps one 1-2 from mouth to mouth for adults.
- Blow gently into their lungs until you see their chest rise. Pay the same consideration as you would to a child under one year old and don’t blow too hard or long.
- Stop, and let the air escape.
- Repeat to give one breath every 3 seconds.
- After 20 breaths check the pulse.
- If absent, start CPR, and if present continue mouth-to-mouth until help arrives.
Cardio-Pulmonary Resuscitation
Adults
- Give two breaths as described above.
- Position the heel of your hand slightly above where the breastbone and the ribs meet.
- Interlock your fingers with your other hand.
- Keep your arms straight and press down firmly, then release but keep your hands in the same position.
- Repeat 15 times.
Note: CPR is physically demanding and, where possible, should be carried out by two people. The two aid-givers should swap roles over 15 compressions.
Children
Baby (under 1 year of age)
- Ensure the baby is on a firm surface.
- Place two fingers slightly below the nipple line in the middle of the chest.
- Press down and release 5 times, at a rate of twice per second.
- Continue mouth to mouth for one breath as described above.
- Repeat steps 3-4 until help arrives.
- If a pulse appears and is above 60 bpm stop the chest compressions but continue ventilation.
Child (over 1 year)
- Place one hand slightly above where the breastbone and ribs meet.
- Use the heel of your hand to press down firmly and release.
- Repeat 5 times at a rate of 2 per second.
- Blow air into the lungs once, as described above.
- Repeat steps 3-4 until help arrives.
- If a pulse is present stop compressions but continue ventilation.
Severe Bleeding
A severed
Even a small cut to an artery can result in huge blood due to the pressure. Suffering from extensive blood loss can lead to shock, unconsciousness or even death. Anything more than a litre of blood from an adult and a third of a litre from a child is considered harmful and the injured person is at risking dying.
The following steps should be used to treat severe bleeding from a limb:
- If conscious, get the person to lie down and try to raise the injured limb, as the elevation will cause a reduced blood flow to the area. This slows down blood loss.
- Press either a clean dressing or, if unavailable, a clean item of clothing, firmly against the wound and maintain the pressure.
- Remove debris, such as glass and metal from the injury site before applying pressure.
- Place a clean dressing over the wound and then apply a bandage to the entire limb.
- Do not remove the dressing if it becomes soaked in blood. Apply a second dressing, up to a maximum of three, and maintain pressure for a further 10 minutes.
- Seek medical attention if bleeding does not stop.
Head Injury
Head injuries can be hard to spot and in many cases, there might not be a visible wound. When this happens you’re going to have to look for other signs that indicate a head injury. Just because you can’t see an injury site, take care as serious head injuries can be fatal. may not always be obvious. Other signs to look for when you suspect a head wound:
- Blood or a straw-coloured liquid seeping from the ear (the latter is a good indication of a fractured skull)
- Unconsciousness
- Dizziness
- Nausea
- Headache
Apply the following treatment to visible head injuries:
- if the wound is open, attempt to pull flaps of skin back in place. In the past, I’ve stitched my own injuries with an emergency first aid kit but only do this if you have a strong stomach, confident or the fix is one of last resort.
- Press a clean dressing firmly on the wound.
- Use a binding, or some other item like a belt to secure the dressing in place.
- If the person is conscious lie them down but raise their head and shoulders.
- If they have fluid leaking from an ear, secure a dressing over it and tilt the person’s head to allow free drainage.
- Severe head injuries can be lethal. Seek medical attention as soon as possible.
Chest Injuries – Punctures
- Reduce the flow of blood from the wound by covering it with a palm.
- Dress the wound and then seal it with a piece of plastic sheet.
- Tie off with either a binding or belt to form an airtight seal.
- if you’re at a high altitude, descend ASAP as thin air makes breathing diffficult and could lead to complications
Internal Bleeding
Internal bleeding is an injury that can be easily missed. When blood vessels are ruptured blood can leak into cavities within the body. This type of injury can be caused by a fracture or even a fairly minor sprain. In some cases, a blow to the body is strong enough to rupture a blood vessel but not the skin.
Some of the signs you should watch out for:
- Constant pain in the affected area
- Cold, clammy skin
- Fainting
- Loss of colour
- Nausea
- Dizziness
- Dilated pupils
- Being out of breath
- An irregular pulse
- Swelling or bruising at the site
Treatment for internal bleeding:
- Seek professional medical treatment immediately
- No drinkgs for the injuted person.
Dislocations
A dislocation is where one or more bones at a joint are removed from its socket. Most commment sites of dislocations include, the shoulder, finger, thumb or jaw (which can be incredibly painful). A disclotion can be recognised by:
- Swelling
- Out of place bones
- Pain and tenderness
- Change in skin colour
To treat, follow these instructions:
- Apply a splint to the joint to prevent movement
- Keep the injured area elevated, if possible
- Do not attempt relocate the joint.
Fractured Forearm
- If the person can hold the arm across their chest then apply a splint and help position it with a wide sling. The person’s fingers should be positioned above their elbow so that the arm forms a ‘V’ shape.
- If the injury prevents the arm from being bent, splint it in the straight position then using a binding, scarf, belt,, ect to secure it to the side of the body.
- Seek medical help.
Other Fractures
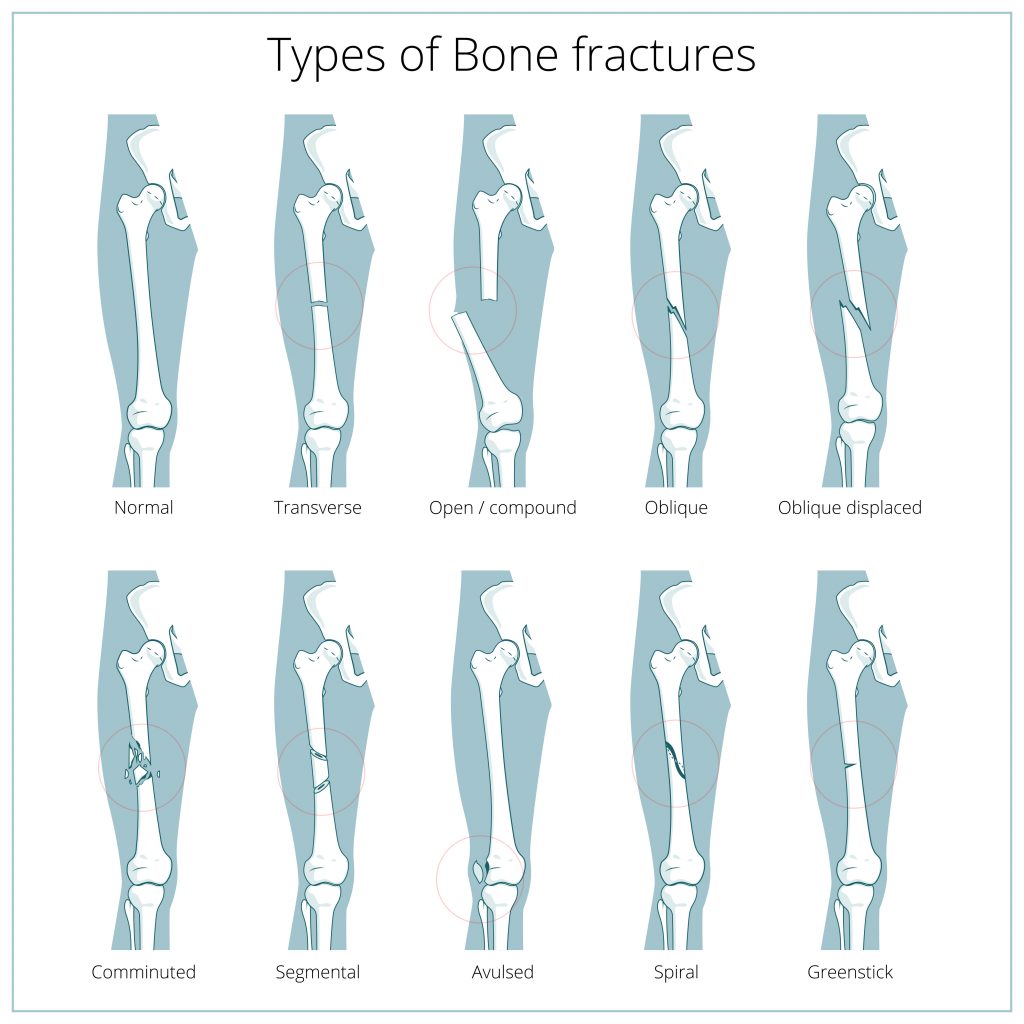
A fracture can be either a broken or cracked bone and there are two types you need to know about; simple and compound. A simple fracture does not break the skin. If left untreated the sharp edges of the broken bone and peirce the skin and developo into a compound fracture (which is where the bone pierces the skin)
A compound fracutre can serious bleeding and presents a high risk of infection and other complications. Signs of a compound fracture include:
- Pain and tenderness
- Difficulty moving
- Difficulty breathing
- Swelling
- Bruising
- Change in skin colour
Treatment for a compound fracture:
- Reduce, or stop any bleeding.
- Cover any open wound with a clean dressing, but do not apply any pressure to the injury.
- Secure the injured limb to a solid part of the body. Use a sling to support fractured arms. If you don’t have a triangualr bandage available, use a piece of clothing to form the sling.
- Watch for signs of shock.
- Warmth is essential, put the person in a sleeping bag if possible.
- Apply a splint (see below).
The Splint
A splint is a method of keeping movement in a fractured bone to a minimum. They are easy to fit, and these steps are simple to follow:
- Simple or compound: check the suspected fracture sight to assess whether it’s simple or compound.
- Blodop flow: does the patient have circulation above and below the fracture? Are they able to move fingers toes (if appropriate)?
- Apply clean dressings to control bleeding.
- Administer pain medication if necessary.
- Apply a splint (which should be placed both above and below the injury).
- To reduce the risk of further damage to the injury site, prepare the splint on an uninjured body part, and then transfer it to the injured area. In addition, this will reduce the amount of pain associated with splinting a fracture limb.
- Be creative when making splints. Sticks, ski poles, tent poles or other similar objects can be used.
- Fastenings can be made from belts, rope, bootlaces, bandages, tape and strips of clothing. Slings can be made from triangular bandages, sheets, and ropes.
- Apply the splint in a way that it does not interfere with circulation – not too tight.
- If you’re in a cold climate, and the fracture is simple with no signs of decreased circulation, pack ice/snow around the wound to hlep reduce swelling and pain. Don’t apply ice directly to the skin, your patient won’t thank you!
- Every 15 minutes after the splint has been applied, check the injury site to ensure that swelling inside the splint has not cut off the circulation.
- Where possible, elevate the injured part to reduce/minimise swelling.
- If you feel the injury is severe, seek medical help. In the case of a broken toe, or finger, it’s possible to go on with your journey once first aid has been applied.
Anyone who has suffered from a broken bone should have a full evaluation once they returen home. Misaligned bones can leads to complications further down the line.
What to avoid:
- Unless necessary, moving the person as this can lead to secondary injuries including damage to internal organs.
- Applying pressure to a compound fracture to stop bleeding – it may cause extreme pain and can move bones.



